
Gene Therapy for OTOF-Mediated Genetic Hearing Loss
The science and story behind the first-ever FDA-approved gene therapy for hearing loss

For most of the history of genetic hearing loss, a diagnosis answered the question of why, but not necessarily the question of what now.
That’s part of why the recent OTOF gene therapy trials have been so important to me personally and scientifically. They represent one of the clearest examples in hearing loss medicine where molecular diagnosis, translational research, surgical innovation, and patient care are all starting to converge in a very real way.
Here, I’ll retrace the steps of how the OTOF story evolved, how groups like Akouos and Regeneron became connected to the Translational Hearing Genomics Laboratory at Boston Children’s Hospital, what the actual science behind the therapies looks like, and why I think this moment matters for the future of hearing loss research.
Why OTOF?
The OTOF gene encodes otoferlin, a protein that is critical for synaptic transmission between inner hair cells and the auditory nerve. In patients with biallelic pathogenic OTOF variants, the inner ear structure is often relatively preserved, but the signaling machinery required for hearing does not function properly.
In simpler terms: the “microphone” of the inner ear can still physically exist, but the signal doesn’t get transmitted correctly.
That distinction is important because it makes OTOF-mediated hearing loss particularly attractive for gene therapy approaches. If the cellular architecture is still intact, then theoretically, restoring functional otoferlin expression could restore physiologic hearing.
That idea moved from theory to reality surprisingly quickly.
How the BCH Translational Hearing Genomics Lab Became Connected to This Work
One thing that often gets lost when people talk about gene therapy breakthroughs is that they usually depend on years of infrastructure and relationship-building that happened long before the headlines. I consider myself extraordinarily blessed to have had the fortune of joining the right lab at the right time.
Specifically, the Translational Hearing Genomics Laboratory Boston Children’s Hospital (BCH) led by Dr. Eliot Shearer has spent years building large hearing loss sequencing cohorts, improving molecular diagnostics, and helping characterize rare forms of hereditary hearing loss. That work has created a foundation that has become increasingly valuable as hearing loss therapies became more genotype-specific.
As companies like Akouos and later Regeneron moved deeper into OTOF therapeutic development, creating relationships with academic hearing genetics groups became increasingly important. Clinical trial recruitment for ultra-rare diseases depends heavily on accurate molecular diagnosis, longitudinal patient characterization, and trusted clinical relationships with families.
Industry couldn’t do it all alone. They needed academia - to identify appropriate patients, to understand natural history, and to connect molecular findings to clinical phenotypes.
That’s part of what I’ve found most interesting about this space. The therapy itself is only one piece. The surrounding ecosystem – from sequencing to diagnostics to counseling to natural history studies to surgical expertise to audiology infrastructure to patient trust – matters just as much.
The Akouos / AK-OTOF Approach
Akouos was one of the first companies to push aggressively into inner ear gene therapy all the way back in 2016, and their differentiator was using adeno-associated virus (AAV)-based approaches for monogenic hearing loss.
Their AK-OTOF program focused on delivering a functional copy of OTOF using an AAVAnc80 vector through intracochlear administration. The core concept was pretty simple: replace the dysfunctional OTOF gene with a functional copy in inner hair cells to restore synaptic signaling and hearing. (Tward et al., 2026)
The delivery approach itself was particularly interesting. Instead of relying on a broad systemic administration strategy, the therapy used direct intracochlear administration with a minimally invasive transcanal approach and the Akouos Delivery Device. (Tward et al., 2026)
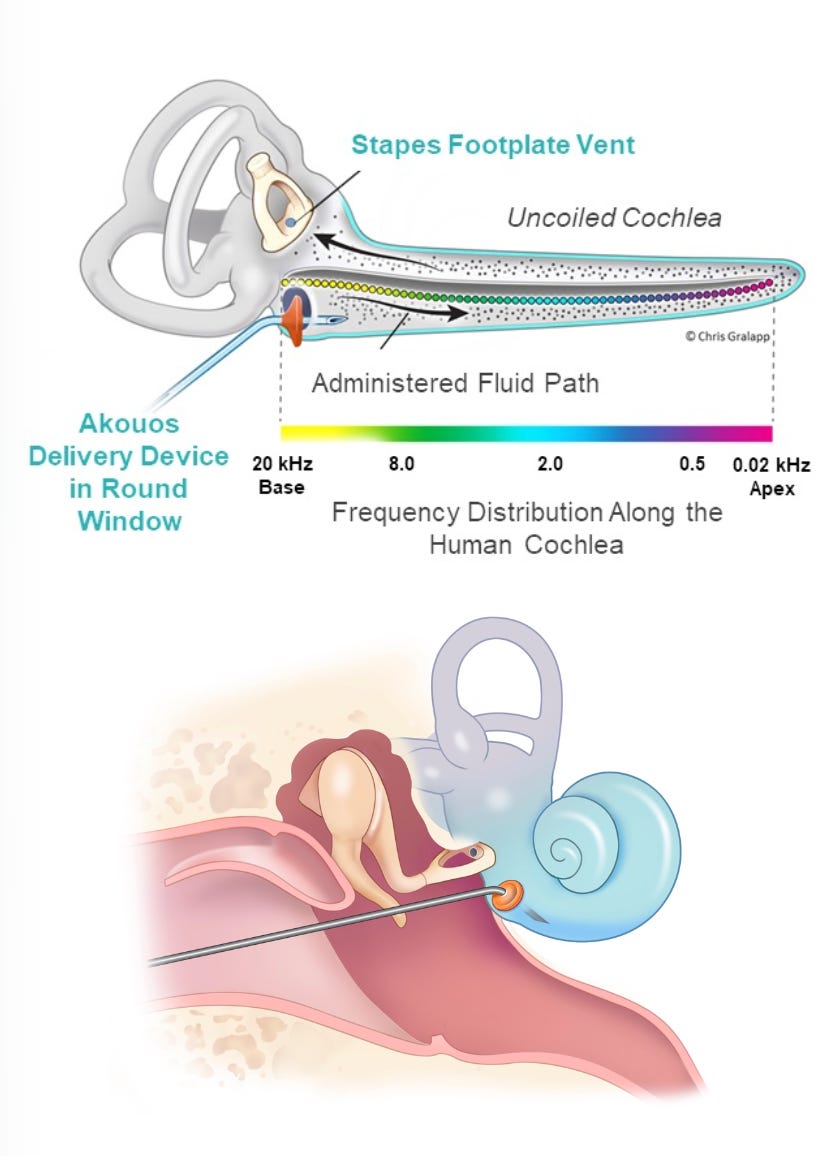
Figure 1: Schematic of AK-OTOF inner ear delivery / intracochlear administration [sourced from Gao et al., 2023]
The early data from AK-OTOF suggested that hearing restoration could begin as early as one month after administration. (Tward et al., 2026)
Regeneron, Decibel, and DB-OTO
In parallel, another branch of this story began developing in 2023 when Regeneron acquired Decibel Therapeutics and continued development of the DB-OTO program.
The DB-OTO approach used a dual AAV1 vector system designed to deliver the large OTOF coding sequence into inner hair cells. Because the OTOF gene exceeds the packaging capacity of a single AAV vector, the therapy uses a dual-vector recombination strategy to reconstruct the full transgene inside the target cells. (Valayannopoulos et al., 2026)
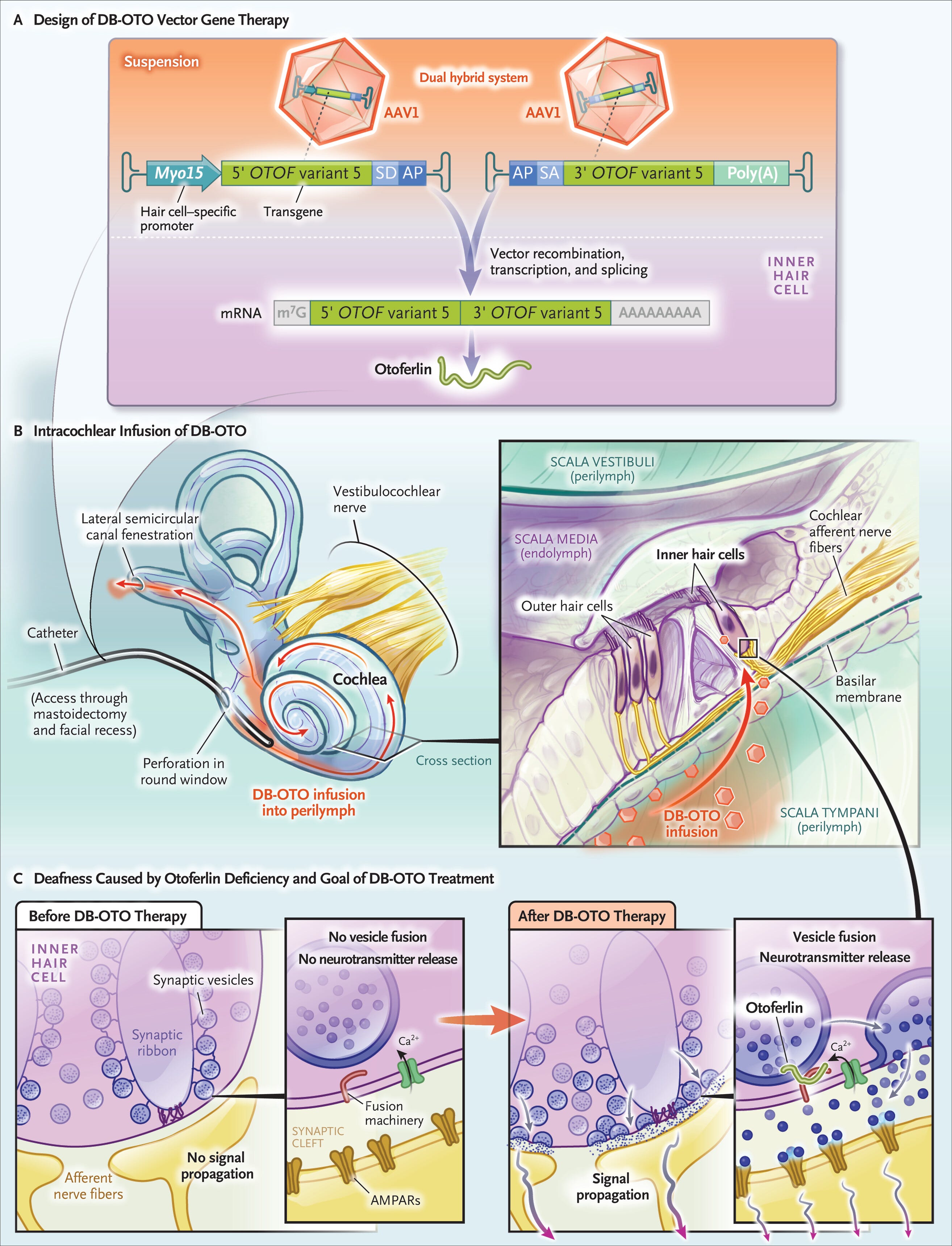
Figure 2: Schematic of DB-OTO inner ear delivery / intracochlear administration [sourced from Valayannopoulos et al., 2026]
The actual surgical delivery method was also important. The therapy was administered through intracochlear infusion that is quite similar to cochlear implant surgery. (Valayannopoulos et al., 2026)
The biological rationale behind DB-OTO was particularly compelling because OTOF-mediated deafness often preserves inner ear cellular architecture despite profound hearing loss. That means the “hardware” of the cochlea can still exist even when synaptic signaling fails.
The actual clinical results were incredible.
In the CHORD trial, 9 of 12 participants achieved the primary efficacy endpoint by week 24, reaching hearing thresholds at or below 70 dB HL after treatment. Several participants reached soft speech sensitivity, and three achieved average normal hearing sensitivity. (Valayannopoulos et al., 2026) (Valayannopoulos et al., 2026)
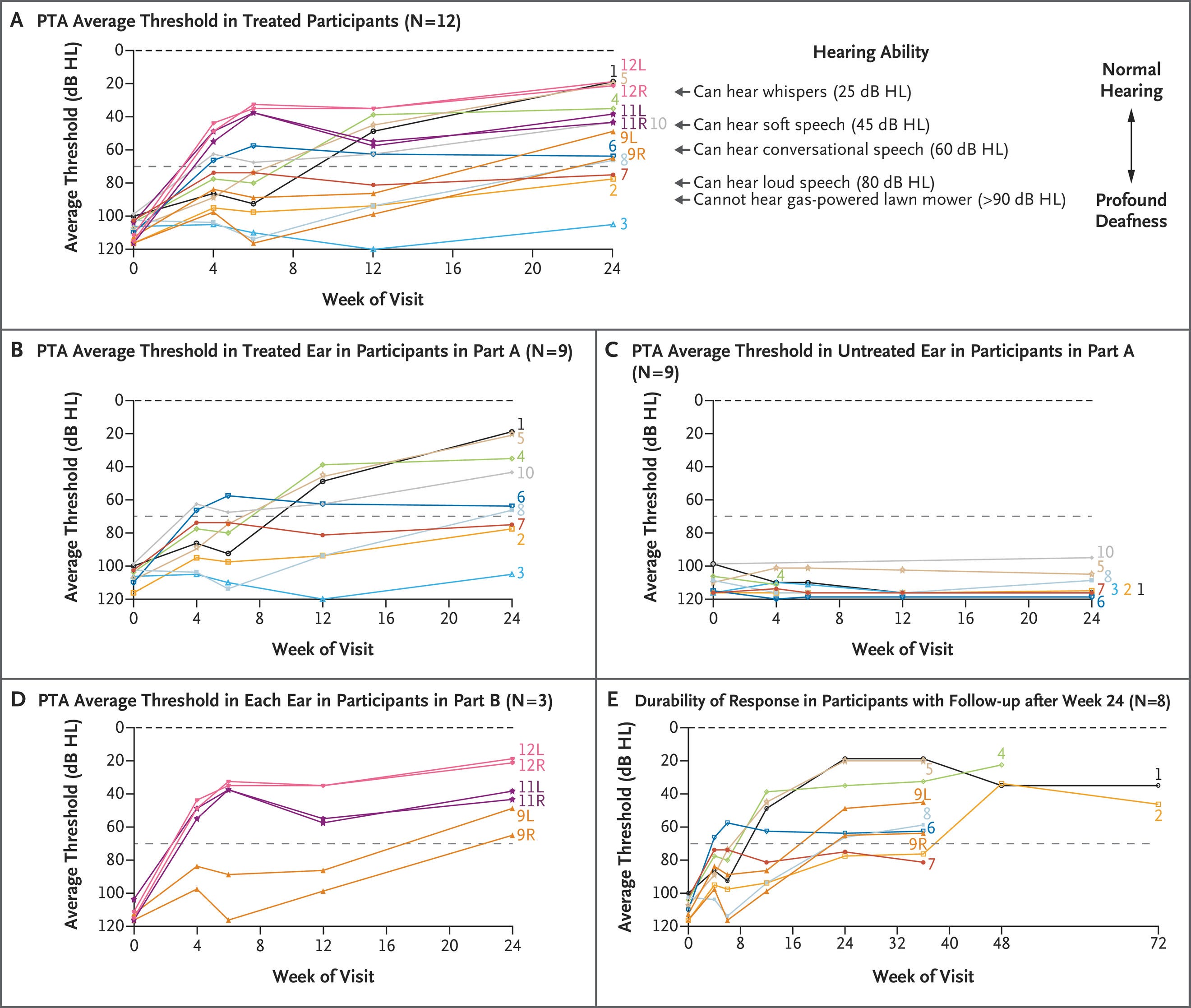
Figure 3: Summary of hearing function recovery in DB-OTO patients [sourced from Valayannopoulos et al., 2026]
One thing I appreciated about the paper was that it did not pretend everything was fully solved. The authors discussed variability in response, the unknowns surrounding durability, and the reality that some participants improved substantially while others improved more modestly or not at all. (Valayannopoulos et al., 2026)
The FDA Approval
Just yesterday, on April 23, 2026, the FDA approved Otarmeni (lunsotogene parvec-cwha), making it the first-ever dual AAV vector-based gene therapy approved for genetic hearing loss. (FDA, 2026)
The approval was significant not only because of the therapy itself, but because it signaled that hearing restoration through gene therapy had moved from experimental concept into real regulatory reality.
The FDA approval specifically targeted patients with severe-to-profound or profound sensorineural hearing loss associated with confirmed biallelic OTOF variants. (FDA, 2026)
The press release also emphasized something that people in hearing genetics have known for a long time: delayed diagnosis matters. If therapies become increasingly genotype-specific, then molecular diagnosis becomes time-sensitive in a way it historically was not. (FDA, 2026)
I think that shift has major implications for the future of hearing loss medicine.
A Big Step Forward but NOT a Universal Solution
I think it’s incredibly crucial to not frame gene therapy as some universal “solution” to hearing loss. Hearing loss is medically, culturally, and personally complex. Deaf and hard-of-hearing identity, accessibility, language, and community still matter deeply regardless of what therapeutic technologies emerge.
But I also think it would be difficult to overstate how meaningful it is that children born with profound OTOF-mediated deafness may now have access to therapies that restore physiologic hearing.
The part I care about most is what this means for families navigating uncertainty. A molecular diagnosis is increasingly becoming more than an explanation. It may become the thing that determines eligibility for treatment, trial enrollment, counseling, and long-term planning.
That changes the importance of diagnostics entirely.
It’s also one of the reasons I remain so interested in long-read sequencing and unresolved hearing loss genomics. The better we become at identifying difficult variants, structural variants, and noncoding causes of hearing loss, the more likely it becomes that patients can actually access therapies that depend on accurate diagnosis.
References
Valayannopoulos V, Bance M, Carvalho DS, Greinwald JH Jr, Harvey SA, Ishiyama A, et al. DB-OTO gene therapy for inherited deafness. N Engl J Med. 2026;394(11):1074–1083. doi:10.1056/NEJMoa2400521. Available at: https://www.nejm.org/doi/full/10.1056/NEJMoa2400521
Tward A, on behalf of the AK-OTOF-101 trial and site teams and Eli Lilly and Company. Preliminary safety and efficacy of AK-OTOF gene therapy for otoferlin gene (OTOF)-mediated hearing loss. Genet Med Open. 2026. doi:10.1016/j.gimo.2026.103685. Available at: https://www.gimopen.org/article/S2949-7744(26)00195-0/fulltext
U.S. Food and Drug Administration. FDA approves first-ever gene therapy for treatment of genetic hearing loss under national priority voucher program [press release]. Silver Spring, MD: U.S. Food and Drug Administration; April 23, 2026. Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-ever-gene-therapy-treatment-genetic-hearing-loss-under-national-priority-voucher